
Masks and plagues have an interesting history that has evolved in lockstep with medical knowledge and the courage of doctors and others to wear them. That history is mirrored by the advances of vaccinations in response to pandemics.
“The history of masks is in many ways a history of epidemiology. The plague doctors of the 17th century had a scary bird mask didn’t prevent anyone from contracting the plague,” writes Sarah Durn, author of The Beginner’s Guide to Alchemy. “The transition from miasma (bad air causes disease) to germ theory was a slow one, but already in the 1800s there was an understanding of the usefulness of face masks in factories.”
Durn’s Cliff’s Notes blog on the history of facemasks for safety is a fascinating read.
As far back as the 16th century, Leonardo da Vinci, who dissected corpses to understand human anatomy, observed inhaled dust and airborne particles were bad for the lungs. However, it took the accumulated death toll of miners and flax spinners to prompt the invention of early respirators by Alexander von Humboldt in 1799. Humboldt was a German naturalist with no medical training who spent time observing underground caverns and mining operations and eventually was hired by Prussian officials to oversee mines. Humboldt also invented the miner’s safety lamp.
Face coverings are mostly to protect others, not yourself, from viral spread. Depending on their quality and design, masks offer some self-protection, but public health officials urge using them to limit transmission of the COVID-19 virus, avoid wider spread and lower the odds of further mutations.
Masks and medicine didn’t click until the 20th century. “The medical world was much slower to adopt the innovation. For nearly 50 years, doctors fought against wearing masks, until the Manchurian plague became a lethal testing ground for the face mask’s importance,” Durn writes.
Dr. Wu Lien Teh, who received his medical training at Cambridge, pioneered the facemask for doctors, nurses and undertakers in the Manchurian plague that broke out in 1910. He was just 31-years-old, faced scorn from his medical colleagues and died from the disease. But his example inspired the use of facemasks during the 1918 Spanish flu epidemic. Facemasks have been a fixture in pandemics involving airborne viruses ever since, though not everyone in our contemporary world is a believer.
One of the first doctors to wear a facemask during surgery was French Dr. Paul Berger in 1897. He initiated the practice after reading Carl Flügge, a German bacteriologist who discovered a link between saliva and disease-causing germs. In 1905, the Journal of the American Medical Association published an article deploring the lack of masks during surgery, including one eyewitness who told of watching a surgeon issue a “continuous spray of saliva” while teaching a medical course and conducting an operation.
In 1906, British Dr. Berkeley Moynihan published a medical textbook, Abdominal Operations, that chastised medical practitioners for failing to don masks and to “scoff at the necessary precautions taken by those who practice aseptic surgery; the meaning of the word ‘aseptic’ is forgotten.” Doctors were still scoffing until 1910 when Wu required his staff to wear masks.
The design of facemasks has taken even longer to evolve. “Throughout the early decades of the 20th century, patents were issued various styles of masks,” Durn says. “Most commonly, masks were made of cotton gauze and held in place with a metal frame. Modern disposable masks grew in popularity in the 1960s. In 1972, the N95 respirator was invented, featuring becoming a healthcare standard in epidemics in 1995.” Perhaps the best current mask is the tightly fitting, five-layer KN95.
Given that doctors resisted facemasks for 50 years, it’s not surprising the public has been variously bewildered and offended by mask mandates, with a segment of the population deciding not to wear a mask as signs of personal freedom and partisan affiliation.
Despite confusing messages during the pandemic, “The evidence in favor of community face coverings to slow the spread of COVID-19 is strong,” writes Dr. John R. Raymond, a nephrologist associated with the Zablocki VA Medical Center in Milwaukee, in an article titled: “The Great Mask Debate: A Debate That Shouldn’t Be a Debate at All”. “There is strong evidence from various laboratory, epidemiological, natural history, clinical and economic studies to support the community use of face coverings to mitigate the spread of COVID-19.”
Therein is the source of public confusion. Face coverings are mostly to protect others, not yourself, from viral spread. Depending on their quality and design, masks offer some self-protection, but public health officials urge using them to limit transmission of the COVID-19 virus, avoid wider spread and lower the odds of further mutations.
The most effective self-protection against contracting the virus is vaccination, which has its own historical narrative and host of critics and skeptics.
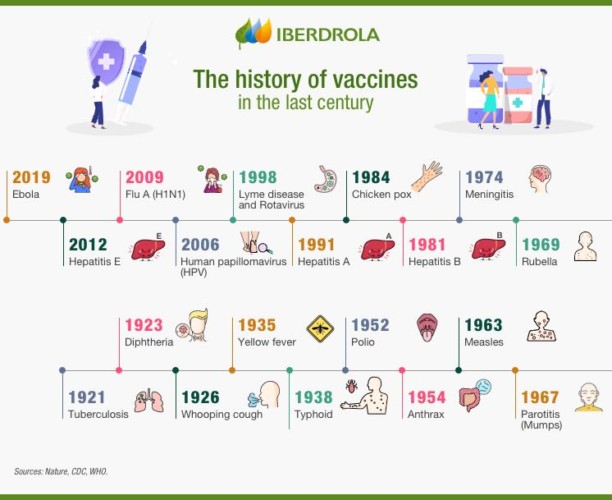
Vaccination dates to Buddhist monks who drank snake venom to gain immunity from snake bites. Vaccination took a leap into the future when Edward Jenner risked reproach in 1796 for inoculating a 13-year-old boy with the vaccinia virus to develop immunity to smallpox. Louis Pasteur experimented with a vaccine for cholera in 1897. Plague vaccine was invented in the late 19th century. Alexander Glenny perfected a vaccine to combat tetanus in 1926 and a pertussis vaccine in 1948. Research between 1950 to 1985 led to the Salk and Sabin vaccines for polio. Later, vaccines were developed for measles and mumps, which once were common childhood diseases.
Molecular genetics has opened the door to an expanding variety of vaccines and vaccine delivery systems for tuberculosis, streptococcal disease, influenza and HIV. Vaccines are on the horizon for allergies, autoimmune diseases and addictions.
There are multiple vaccines authorized for emergency use to combat COVID-19, which clinical tests and mass vaccinations have shown as very effective in protecting people from contracting the virus. Final approval for the Pfizer COVID-19 vaccine is pending before the Federal Food and Drug Administration. The bio-engineered mRNA COVID-19 vaccines are blazing the way for rapid development of new vaccines for known and future diseases, as well as unprecedented mass production and the ability to adjust vaccines to address viral mutations.
In politics, masks and COVID-19 vaccines have been fused together, blurring their respective purposes: Masks are intended to protect others; vaccination is meant to protect yourself. It would be useful if there at least was broad public agreement on that point.



